

Remote monitoring in healthcare is split into two key services: Remote Physiological Monitoring (RPM) and Remote Therapeutic Monitoring (RTM). Here’s what you need to know:
- RPM tracks objective physiological data (e.g., heart rate, blood pressure) using FDA-approved devices that automatically transmit data. It’s typically used for chronic condition management and billed by physicians or mid-level providers.
- RTM focuses on subjective therapeutic data (e.g., pain levels, therapy adherence), often input manually by patients via FDA-cleared apps or devices. RTM is broader, allowing therapists (physical, occupational, speech-language) to bill for these services.
Key updates for 2026:
- New "rescue codes" allow billing for shorter monitoring periods (2–15 days), replacing the previous 16-day rule.
- RPM and RTM cannot be billed for the same patient in a 30-day period.
Both programs require compliance with Medicare rules, proper documentation, and regular data review. RPM suits chronic condition monitoring, while RTM supports therapy adherence and recovery tracking.
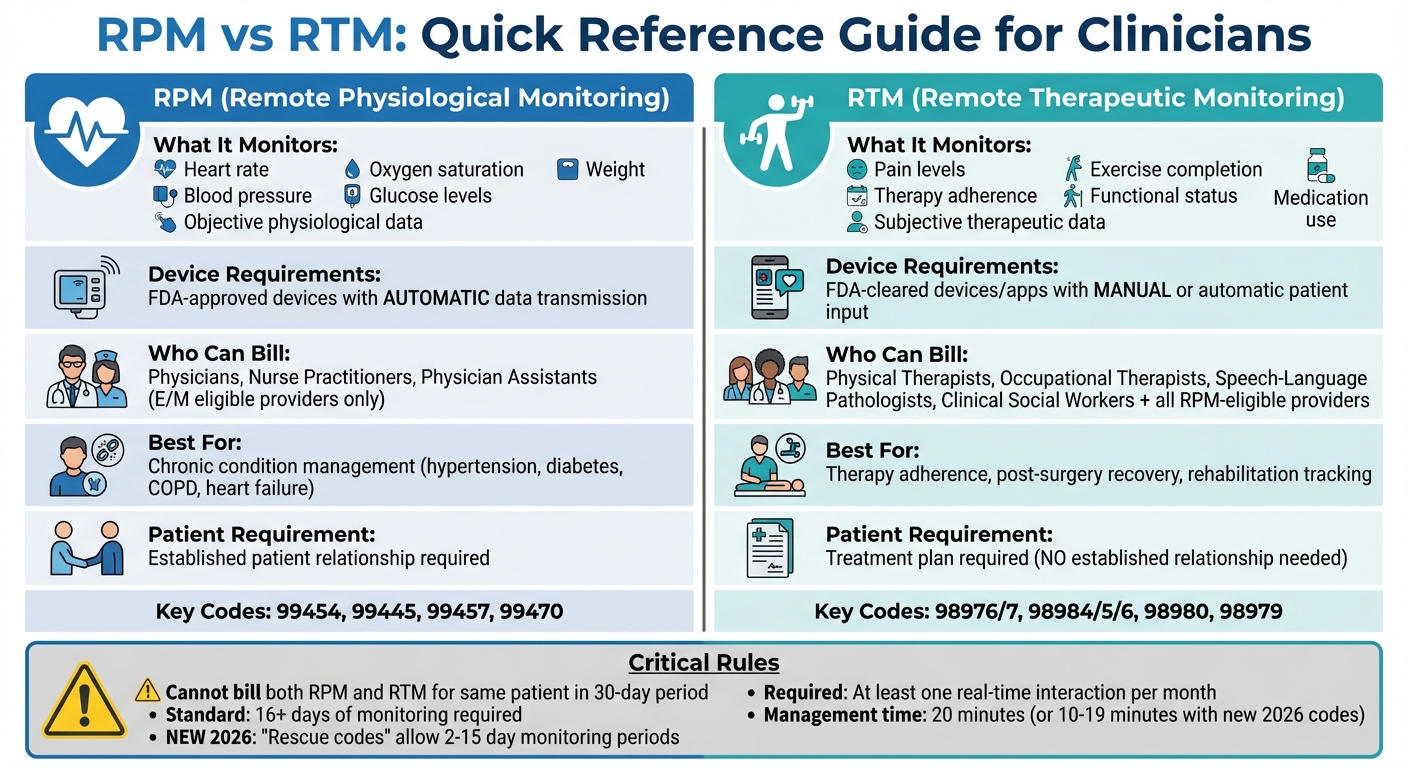
RPM vs RTM Remote Monitoring Comparison Chart for Healthcare Providers
What’s the difference between Remote Therapeutic Monitoring and Remote Patient Monitoring?
sbb-itb-44aa802
How RTM and RPM Differ
The key difference between Remote Therapeutic Monitoring (RTM) and Remote Physiologic Monitoring (RPM) lies in what they measure and who is qualified to deliver care under each program. RPM focuses on tracking objective physiological data – like blood pressure, heart rate, oxygen saturation, glucose levels, weight, and respiratory flow rate. This data must be automatically transmitted from an FDA-cleared medical device. On the other hand, RTM gathers therapeutic data – such as exercise adherence, pain levels, and functional status – through patient-reported inputs recorded via an FDA-cleared medical device or Software as a Medical Device (SaMD).
Their goals also set them apart. RPM aims to identify and address potential health crises early. For example, monitoring a heart failure patient’s daily weight can help prevent hospital readmissions. RTM, however, evaluates treatment effectiveness and patient compliance. A physical therapist might use RTM to track how well a patient is following a post-surgery exercise program or to monitor pain levels, adjusting the rehabilitation plan as needed. Below, we’ll break down what each program monitors and who can bill for these services.
What Each Program Monitors
RPM focuses on automated data transmission. Devices like connected blood pressure cuffs automatically upload readings without requiring manual input. This automation is a strict requirement for RPM billing and ensures clinicians have the data they need to make timely decisions.
RTM tracks treatment adherence and response beyond vital signs. This includes details like how often a patient performs prescribed exercises, self-reported pain levels, use of rescue inhalers, and evaluations of musculoskeletal or respiratory conditions. Unlike RPM, patients can manually input this information via an app or device, as long as the tool qualifies as an FDA-cleared medical device or SaMD. However, generic wellness apps or simple text messaging platforms don’t meet the criteria for billing.
Who Can Bill for Each Service
RPM billing is restricted to physicians and certain non-physician practitioners – such as nurse practitioners and physician assistants – who are eligible to bill for Evaluation and Management (E/M) services.
RTM, on the other hand, allows a broader range of providers to bill. This includes physical therapists, occupational therapists, speech-language pathologists, and clinical social workers, alongside the providers eligible for RPM billing. The Centers for Medicare & Medicaid Services (CMS) specifically designed RTM codes to support rehabilitation and therapy professionals.
It’s important to note that you can’t bill for both RTM and RPM for the same patient within a 30-day period. The choice between the two depends on the type of monitoring required and the expertise of your care team. For therapists billing RTM, they must use the proper therapy modifiers (GP for physical therapy, GO for occupational therapy, or GN for speech-language pathology) and maintain an active, certified plan of care.
Technology and Device Requirements
To maintain compliance and avoid billing errors in RTM and RPM programs, it’s crucial to understand the specific technical requirements for each type of monitoring. Here’s a breakdown of the device criteria for both.
FDA-Approved Devices for RPM
For RPM, only medical devices that meet the FDA’s definition under the Federal Food, Drug, and Cosmetic Act are acceptable. These devices must automatically collect physiological data and securely transmit it without requiring any manual input from patients. Examples include blood pressure cuffs, pulse oximeters, digital scales, glucometers, and continuous glucose monitors (CGMs), all of which must send data directly to your system.
This automation ensures accurate data collection and enables clinicians to quickly detect changes in a patient’s health. For instance, a connected blood pressure monitor used for managing hypertension can send readings throughout the day, giving a complete view of the patient’s cardiovascular health. To stay compliant, ensure devices like FDA-cleared blood pressure monitors securely transmit data for at least 16 days per billing period and integrate seamlessly with your EHR system.
Patient-Reported Tools for RTM
RTM offers greater flexibility in device selection. These tools can include software applications, wearable sensors, or digital platforms that allow patients to manually input therapeutic data. This might involve apps for tracking exercise, logging pain levels, or monitoring inhaler usage. Unlike RPM, RTM devices or Software as a Medical Device (SaMD) can incorporate patient-reported outcomes (PROs).
For example, in musculoskeletal monitoring, wearable sensors like the aiSpine device can track posture in real time, provide vibration reminders for adherence, and monitor progress. Similarly, the aiRing monitoring ring captures therapeutic data in various conditions with its waterproof design and intelligent touch controls, making it suitable for daily use. Both devices work with the AIH Health App, offering historical data analysis and personalized feedback, and meet the FDA’s medical device definition required for RTM billing.
The key is ensuring that your chosen platform qualifies as an FDA-cleared medical device or SaMD and allows clinical staff to efficiently review patient-reported data within your EHR workflow.
Patient Selection and Enrollment
Choosing the right patients is just as important as selecting the right devices when it comes to successful remote monitoring. The foundation of effective monitoring lies in enrolling patients based on their clinical needs. Remote Patient Monitoring (RPM) is ideal for individuals who require continuous, objective data tracking – such as heart rate, blood pressure, oxygen saturation, or weight. On the other hand, Remote Therapeutic Monitoring (RTM) focuses on therapy adherence and self-management. RPM is particularly helpful for patients managing chronic conditions like hypertension, diabetes, COPD, or heart failure, where quick treatment adjustments can make a big difference. For example, one study involving 1,380 high-risk patients monitored during the first 30 days post-hospital discharge showed that telemonitoring reduced the combined rate of readmissions or deaths from 23.7% to 18.2%. Below are guidelines for selecting candidates for RPM and RTM.
Selecting Patients for RPM
RPM works best for patients at risk of sudden changes in their health who require close monitoring. For instance, individuals with heart failure who need daily weight checks or diabetics requiring frequent glucose tracking are excellent candidates. Medicare rules also require that an established patient relationship exists before enrollment. Additionally, ensure patients have reliable connectivity and are committed to using the device for at least 16 days within a 30-day period.
When to Use RTM Instead
RTM is better suited for patients with stable vital signs who need support with therapy adherence and tracking symptoms like pain or posture. This includes people recovering from back surgery, patients in physical therapy for musculoskeletal issues, or those managing respiratory therapy with inhalers. RTM allows patients to self-report details like pain levels and medication use. For example, a patient recovering from back surgery with stable vitals but needing posture monitoring and exercise tracking could benefit from RTM devices like aiSpine, which provides real-time posture feedback. Unlike RPM, RTM does not require an established patient relationship for Medicare billing, making it easier to initiate for new therapies.
Data Review and Clinical Response Protocols
Once devices are live, it’s essential to review the data regularly and act without delay. Most RPM (Remote Patient Monitoring) and RTM (Remote Therapeutic Monitoring) platforms prioritize patient lists by alert severity, helping clinicians focus on the most critical cases first. These platforms streamline the review process, but having a monitoring management plan tailored to each patient’s specific condition, comorbidities, and risk level is equally important. Whether a patient is in an acute, post-acute, subacute, or chronic phase, the plan should define how often data is reviewed and how interventions are handled.
How Often to Review Data
The frequency of data review depends on the patient’s risk level. High-risk patients often benefit from daily monitoring, while those with stable chronic conditions may only need a review every few days. On the other hand, patients in acute or post-discharge phases might require twice-daily check-ins. A mid-cycle review around day 15 can help identify patients who might fall short of the 16-day monitoring threshold. This is especially important with the introduction of the 2026 "rescue codes" (98984–98986), which allow billing for monitoring periods as short as 2–15 days.
Medicare also requires at least one real-time interaction – via phone or video – with the patient or caregiver each calendar month to meet the criteria for certain management codes like 98980 (RTM) or 99457 (RPM).
When to Intervene and How to Document
After establishing review schedules, the next step is defining when and how to intervene. For example, a single elevated reading might warrant a retest, while patterns like worsening pain or increased use of rescue inhalers could indicate the need for therapy adjustments. Before taking any action, validate patient-reported data to ensure accuracy. This could involve a quick phone call to clarify symptoms or rule out issues like improper device use.
Accurate documentation is critical, especially during audits. Records should include the date, time, and mode of every real-time interaction, along with a summary of the data reviewed and any updates to the care plan. For instance, if a patient’s aiSpine device shows poor posture adherence and increasing back pain, document the conversation where you discussed exercise adjustments and scheduled a follow-up.
"The more explicitly you connect RTM data to care-plan changes, the stronger your position in an audit".
To stay audit-ready, maintain a monthly audit packet that includes the original order, device details (confirming FDA medical device status), timestamped day-count reports, and a log of live interactions. For shift changes or patient handovers, use the ISBAR framework (Identify, Situation, Background, Assessment, and Recommendation) to ensure smooth transitions.
Lastly, track time incrementally throughout the month. With the new 2026 codes for 10–19 minute management sessions (98979 for RTM and 99470 for RPM), shorter interactions – like responding to a single alert or conducting a brief check-in – can now be billed, making it easier to align with real-world workflows.
Compliance and Billing Requirements
Meeting Medicare’s requirements for documentation and billing requires meticulous attention to detail. The Office of the Inspector General has called for increased oversight of Remote Patient Monitoring (RPM) in Medicare, signaling the possibility of stricter audits. To stay prepared, clinicians must maintain audit-ready records that include the beneficiary’s details, the date of service, and the provider’s information on every page.
Medicare Documentation Standards
Medicare requires patient consent to be documented when RPM or Remote Therapeutic Monitoring (RTM) services are initiated. Records must also confirm the use of an FDA-approved, internet-connected medical device capable of transmitting patient data. Standard billing for RPM involves data collection for at least 16 days within a 30-day period. However, new billing codes for 2026 (99445 for RPM and 98984–98986 for RTM) allow for shorter monitoring periods of 2 to 15 days, making them suitable for post-discharge or acute care scenarios.
To establish medical necessity, clinicians must document the acute or chronic condition being monitored. Logs of non-face-to-face services should reflect the time increments billed – whether 10 or 20 minutes. Records should also include patient education on device setup, instructions for use, and recommended usage frequency. Treatment management documentation must detail the review of transmitted data, clinical decisions made, and any follow-up discussions with the patient. For those using Electronic Health Records (EHR), a documented process for electronic signatures is crucial for compliance.
These documentation standards form the groundwork for the billing practices outlined below.
Billing Codes and Restrictions
Certain restrictions apply when billing for RPM and RTM services. For instance, both services cannot be billed for the same patient within the same 30-day period. Additionally, only one practitioner can bill for RPM or RTM services per patient during that time, even if multiple devices are used. While RPM requires an established patient relationship, RTM does not – but both require thorough documentation to ensure compliance.
For 2026, new 10-minute treatment management codes (99470 for RPM and 98979 for RTM) are valued at 0.31 work RVUs, which is about half the value of the existing 20-minute codes. The setup and education code 99453 now requires at least 2 days of monitoring for reimbursement eligibility. These updates highlight the importance of efficient monitoring and detailed record-keeping to meet reimbursement criteria.
When billing RPM or RTM alongside Chronic Care Management (CCM) or Behavioral Health Integration (BHI), practitioners must document the time and effort for each service separately to avoid double-counting. Practitioners receiving global surgical payments cannot bill for RPM or RTM during the global period. However, those who do not receive such payments – like physical therapists – may bill for these services.
The table below summarizes the key service types, codes, descriptions, and requirements:
| Service Type | Code | Description | Requirement |
|---|---|---|---|
| RPM Supply | 99454 | Device supply/transmission | 16+ days of data / 30 days |
| RPM Supply | 99445 | Device supply/transmission | 2–15 days of data / 30 days |
| RPM Management | 99457 | Treatment management | 20 minutes |
| RPM Management | 99470 | Treatment management | 10–19 minutes |
| RTM Supply | 98976/7 | Respiratory/Musculoskeletal supply | 16+ days of data / 30 days |
| RTM Supply | 98984/5/6 | RTM supply codes | 2–15 days of data / 30 days |
| RTM Management | 98980 | Treatment management | 20 minutes |
| RTM Management | 98979 | Treatment management | 10–19 minutes |
Combining RTM and RPM with Other Care Programs
Remote monitoring can work smoothly alongside other care programs, creating a more integrated approach to patient care. Medicare allows clinicians to bill for Remote Patient Monitoring (RPM) or Remote Therapeutic Monitoring (RTM) in combination with programs like Chronic Care Management (CCM) and Behavioral Health Integration (BHI), as long as the time and effort for each service are documented separately. This opens the door to better care coordination and additional revenue streams. Below, we’ll explore how these programs can work together to improve patient outcomes and reimbursement opportunities.
Using RTM and RPM with CCM
Chronic Care Management provides monthly support, including care planning, medication reviews, and coordination. RPM and RTM complement this by offering continuous monitoring between office visits. For instance, if RPM detects a sudden spike in a patient’s blood pressure, it can trigger a priority CCM call or prompt an adjustment to the care plan.
"By embedding RPM within CCM workflows – and supporting provider training, compliance, and operational follow-through – you transform reporting into real-time, high-impact care." – Connor Danielowski, COO, Chronic Care Staffing
Under general supervision, clinical staff like nurses or medical assistants can manage coordination for both programs. They can review device data or reach out to patients without requiring the physician to be immediately available. However, it’s important to note that RPM and RTM cannot be billed for the same patient within the same 30-day period. This integration not only simplifies care coordination but also creates opportunities for better reimbursement strategies.
Increasing Reimbursement Opportunities
By incorporating remote monitoring into existing workflows, practices can unlock greater revenue potential. Research has shown that RPM can reduce hospital admissions, shorten stays, and decrease emergency visits in nearly half of the studies reviewed. These benefits translate into cost savings while generating revenue through various reimbursement codes. In fact, RPM and CCM reimbursement rates are expected to increase by 7% to 21% by 2026.
The updated 2026 billing codes also allow for shorter monitoring periods, which adds flexibility in post-discharge and acute care settings. This makes it easier to pair RPM and RTM with CCM and BHI services. RTM, in particular, is useful for behavioral health integration because it tracks non-physiological data like medication adherence and therapy progress. For example, CPT code 98978 covers RTM monitoring for cognitive behavioral therapy (CBT). When used alongside BHI’s foundational code, 99484 – which requires at least 20 minutes of team-based coordination each month – practices can address both physical and mental health needs while optimizing reimbursement.
The secret to success lies in precise documentation. When billing for CCM alongside RPM or RTM, ensure that time logs clearly separate activities for each program to avoid overlapping minutes. Combining RTM and RPM with other care programs not only enhances clinical workflows but also supports better patient outcomes and compliance.
Staff Training and Preparation
For Remote Therapeutic Monitoring (RTM) and Remote Patient Monitoring (RPM) to succeed, staff training needs to combine clinical expertise with operational precision. Launching these programs requires a well-rounded approach to training. Team members must understand updated clinical protocols, including how to identify and enroll patients, as well as manage data monitoring workflows. Clinicians also need to recognize clinically important data and know when to escalate concerns. Administrative staff should be trained on handling device-related tasks like distribution, tracking, cleaning, and calibration.
"You have to intimately understand and appreciate how a process works from the perspective of the patient, providers and caregivers and each operational stakeholder before you can improve or replace it." – Omid Toloui, Vice President of Digital Health, CareMore
Staff training should also cover the relevant CPT codes for RPM (99453–99458) and RTM (98975–98981), including the 16-day data collection rule. IT representatives must be involved in workflow planning to ensure technical training is thorough and that systems integrate seamlessly with electronic health records. Contingency plans should be in place for addressing data anomalies or emergencies, and automation options for flagging critical data should be explored to streamline processes. Lastly, clinicians need targeted training to interpret and act on the data effectively.
Training Clinicians to Use the Data
Clinicians should understand the difference between physiologic data (e.g., blood pressure, glucose levels) collected through RPM and non-physiologic data (e.g., therapy adherence, pain levels) monitored via RTM. Training should focus on three key areas: Education and Setup, Device Supply (data transmission), and Treatment Management. Notably, treatment management codes do not require the 16-day data collection period.
"Education about how to use the device and transmit the health data helps ensure that patients use the device appropriately to collect accurate data." – CMS
Clinicians must also document non–face-to-face time in 20-minute increments for treatment management, ensuring no overlap when billing for concurrent services. Clear protocols for screening and analyzing data will help the team operate within their full scope. For RPM, patients need to be "established" (having received professional services within the past three years), while RTM requires an established treatment plan but not an established patient relationship. It’s equally critical to ensure patients are well-trained in using their devices.
Teaching Patients to Use Devices
Patient education should occur at multiple points: during an initial telehealth session, through written instructions (handouts or emails), and in a follow-up appointment after several days of device use. A hands-on setup visit is vital for confirming medical necessity and training patients on devices like tablets, wearables, scales, or pulse oximeters. Patients need to understand how their device works, what data it collects, how the data is transmitted, and how it will influence their treatment plan.
Provide patients with printed or digital troubleshooting guides for common issues, such as connectivity problems or device malfunctions. Include family members or caregivers in the training if they will assist with tasks like charging devices or applying sensors. After the first data transmissions, follow up with patients to confirm that data is being received correctly. Tailor training to each patient’s technological comfort level, offering additional support for older adults or those with limited health literacy. Well-prepared patients contribute to more accurate data collection and better treatment outcomes, strengthening the overall remote monitoring strategy.
Conclusion
Implementing RTM and RPM successfully hinges on understanding their key differences and applying strategies that ensure compliance, efficiency, and patient satisfaction. RPM focuses on collecting objective physiological data – like heart rate, blood pressure, or oxygen levels – through automatic device transmissions. Meanwhile, RTM emphasizes patient-reported outcomes, such as pain levels or respiratory activity, and tracks therapeutic adherence. RPM is ideal for managing chronic conditions requiring continuous monitoring, such as diabetes, hypertension, or heart failure. On the other hand, RTM works best for cases like asthma management, post-operative recovery, or cognitive-behavioral therapy, where tracking therapeutic responses is critical.
Accurate documentation is a cornerstone of these programs. Traditionally, both required at least 16 days of data collection in a 30-day period. However, new 2026 codes (98984–98986) now allow billing for shorter monitoring periods of 2–15 days. Management codes also demand at least 20 minutes of clinical staff time and one real-time, synchronous interaction per month. To ensure compliance, documentation must include device details, timestamped day-count reports, and logs of management time. Keep in mind, RTM and RPM cannot be billed simultaneously for the same patient within a 30-day window.
Preparedness is everything. Clinicians need to clearly distinguish between physiological and non-physiological data, document non–face-to-face time accurately, and establish clear protocols for escalating urgent findings. Patients should receive hands-on training with their devices, written troubleshooting guides, and follow-ups to confirm data is being transmitted correctly.
FAQs
How do I choose RTM vs RPM for a patient?
When choosing between RTM (Remote Therapeutic Monitoring) and RPM (Remote Patient Monitoring), it all comes down to your clinical objectives and the type of data you need.
RPM is designed to monitor physiological data, such as vital signs, which makes it a great tool for managing chronic conditions like hypertension or diabetes. On the other hand, RTM zeroes in on therapy adherence and symptom management, gathering information related to treatments such as medication usage or physical therapy progress.
While these two approaches can complement one another, they serve distinct roles and follow different billing guidelines, so it’s essential to understand their unique purposes before deciding which fits your needs.
What qualifies as an FDA-cleared device or app for billing?
Devices or apps cleared by the FDA for billing purposes must qualify as validated medical devices or approved Software as a Medical Device (SaMD). They are required to automatically collect and transmit physiologic data – self-reported data alone does not meet the standards for FDA clearance. These tools play a critical role in ensuring regulatory compliance and enabling precise billing for remote patient monitoring and related therapeutic services.
How do the 2026 “rescue codes” change the 16-day rule?
The 2026 "rescue codes" bring a major update to RTM billing: the removal of the 16-day minimum requirement. Clinicians can now bill for monitoring periods ranging from 2 to 15 days. This shift replaces the old 16-day rule, providing more flexibility in how RTM services are managed and billed.